Notice of West building lobby closure at Lucile Packard Children’s Hospital Stanford
Pediatric Hydrocephalus Treatments
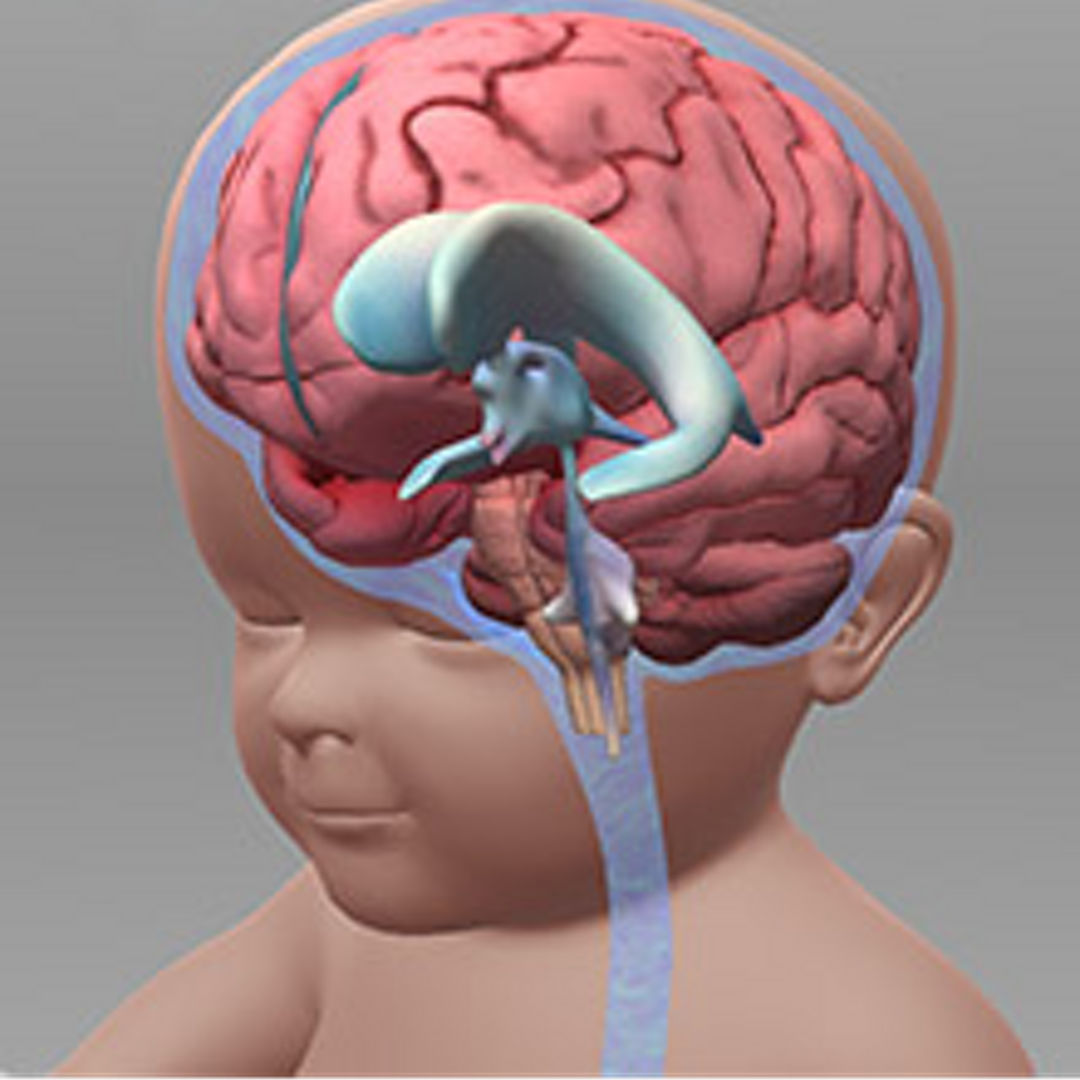
Lucile Packard Children’s Hospital Stanford is a world leader in hydrocephalus treatment, one of the most common brain disorders among newborns and infants. Hydrocephalus results from a buildup of cerebrospinal fluid (CSF) in the brain and spinal column, which can enlarge the heads of newborns and very young children and put pressure on sensitive brain tissue. Left untreated, hydrocephalus can cause serious health and cognitive problems.
Fortunately, most cases of hydrocephalus can be safely and effectively treated. At Packard Children’s, surgeons have pioneered an innovative way of addressing this condition called an endoscopic third ventriculostomy, or ETV. For many young patients, this new procedure represents a significant improvement over previously available hydrocephalus treatments. While traditional procedures have been reliably performed since the 1950s, they require the permanent insertion into the brain of a synthetic tube, called a shunt. That shunt can provoke infection and too often needs to be replaced or repaired later on in the patient’s life. Endoscopic third ventriculostomy, on the other hand, is a one-time procedure that leaves no hardware inside the patient. Packard Children’s surgeons, who serve on the medical advisory board of the National Hydrocephalus Association, are highly rated for both procedures. Whether ETV or the installation of a shunt is the best procedure for any given patient depends on his or her specific diagnosis. But when appropriate, ETV minimizes discomfort and risk while maximizing a patient’s chance of leading an active, independent and healthy life. Learn more with the interactive 3-D animation that illustrates the condition and two main treatments of hydrocephalus.
A plan for pediatric hydrocephalus treatment
Hydrocephalus can occur at different stages of development. Obstetricians regularly take fetal head measurements during pregnancy, and many prenatal cases are first identified that way. When an in utero hydrocephalus patient is referred to them, Packard Children's pediatric neurosurgeons meet with the family to develop a safe delivery plan and discuss the options for hydrocephalus treatment after birth. On the other hand, when a child contracts the condition after birth, his or her pediatrician is typically the first to recognize it. In either case, it is important that the best available experts quickly investigate the source of a patient’s hydrocephalus and chart the best course forward.
At Packard Children’s, doctors employ the latest MRI technologies as well as traditional examination techniques in their diagnosis of hydrocephalus. For example, fast MRI scanners are commonly used for both diagnosis and follow-up of hydrocephalus patients and have largely replaced the far slower traditional CT scanners, which require sedation and entail exposure to radiation.
ETV allows faster, safer return to normalcy
Endoscopic third ventriculostomy (ETV) restores the natural flow of cerebrospinal fluid by creating an opening in one of the ventricles through which CSF is able to flow to the base of the brain. The surgery, enabled by several methodological and technical advances (including the use of a tiny guided camera called an endoscope), takes less than an hour to complete. After putting a patient to sleep with general anesthesia, the surgeon makes a small opening in the frontal area of the skull and guides a remote-controlled instrument through the incision and into the ventricular system. Once the tool is in place, the surgeon creates a small drainage opening, usually in the floor of the third ventricle. A tiny balloon is inserted into the new opening and then inflated to stretch it. After a moment, the balloon is deflated and withdrawn, leaving behind an opening precisely calibrated to permit CSF to flow out at just the right rate, relieving pressure on the brain and slowing the rate of head size growth to normal.
After the free flow of CSF has been restored, in some cases the ETV may be improved further with a procedure called a choroid plexus coagulation (CPC). Cerebrospinal fluid is made by the choroid plexus, a weblike formation of cells that extends along the inner edge of the ventricles and looks something like a fluffy feather boa. Using an endoscope, the surgeon guides an instrument to the choroid plexus and trims it, decreasing the production of CSF in the brain.
Once the CSF in the ventricular system has been diverted and, if necessary, the choroid plexus has been trimmed, the surgeon removes the instruments and closes up the small incision. If all goes as expected, that will be the last brain surgery the patient ever needs to treat his or her hydrocephalus. After an ETV, there is immediate relief from the extra pressure in the brain, and the ventricles gradually decrease in size and head growth normalizes. Most patients spend only one or two days in the hospital for observation and typically can return to regular activity in about two weeks.
Traditional shunt procedure requires implant
An alternative procedure for treatment of hydrocephalus, also performed at Packard Children’s, requires the installation of a piece of synthetic tubing known as a ventricular peritoneal shunt, which drains excess CSF from the brain to the abdomen. As with ETV, the surgeon makes a hole in the patient’s skull through which they navigate one end of the shunt into the ventricular system. The other end is then guided under the patient’s skin, down the neck and typically into the abdomen, where it floats freely in the area surrounded by the organs. Excess CSF flows from the brain into the body cavity, where it is naturally absorbed. A valve on the shunt regulates the flow of CSF through the tubing, letting a patient’s doctor monitor and adjust the CSF pressure. Typically placed behind the patient’s ear or at the back of the neck, the valve also has a small chamber from which cerebrospinal fluid can be periodically sampled for biomarkers of infection or other problems inside the brain. Sometimes the surgeon also inserts a wireless reprogrammable valve that makes it much easier to adjust CSF drainage as the patient grows.
Once the shunt and valve are in place, the surgeon closes up the incisions. As with ETV, the entire procedure typically takes about an hour. Most patients remain in the hospital for a couple of days to ensure that the shunt is working properly and that the areas around it are free of infection. Every child with a history of hydrocephalus needs to be tracked after surgery. Annual clinical visits typically include a fast MRI scan and a neurological exam. Packard Children’s team is equipped to monitor and treat hydrocephalous patients safely from diagnosis into adulthood.
Packard Children’s surgeons successfully treat hydrocephalus with both ETV/CPC and shunt procedures, but a growing percentage of patients are being treated with ETV/CPC. It minimizes the likelihood of infection or other complications, reduces the amount of time spent recovering in the hospital and eliminates the need for more brain surgeries later in life. Whichever procedure is most appropriate for a child with hydrocephalus, Packard Children’s doctors are equipped to give them the best available care.

Connect with us:
Download our App: