Notice of West building lobby closure at Lucile Packard Children’s Hospital Stanford
About Pediatric Hydrocephalus
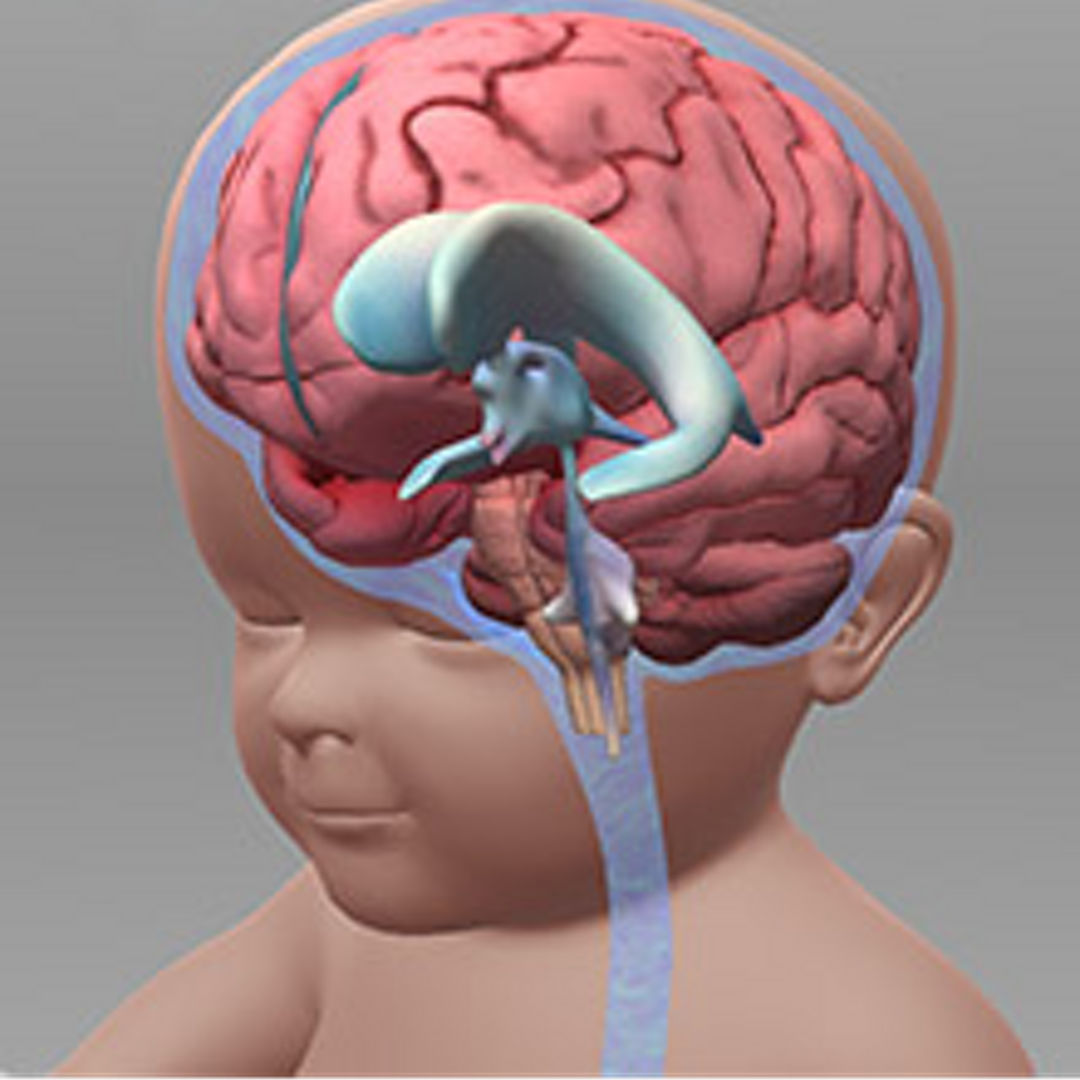
Hydrocephalus is a condition resulting from an overabundance of cerebrospinal fluid in the brain. It is one of the most common childhood brain disorders; 1 in every 500 babies in the United States is born with hydrocephalus, and each year another 6,000 children develop it before they turn 2 years old.
The word “hydrocephalus” is a fusion of the Greek words for “water” and “head.” The “water,” refers to the clear, water-like cerebrospinal fluid (CSF) that normally nourishes, maintains and protects the brain. When the flow or drainage of that fluid is impeded, or when the brain makes too much, the resulting buildup of pressure can both enlarge an infant’s head and put pressure on sensitive brain tissue. A few decades ago, a diagnosis of hydrocephalus may have been grave. Today, if properly diagnosed, the condition is quite treatable.
The function of fluid in the brain
The central nervous system (CNS), composed of the brain and the spinal cord, is the human body’s main command center. It is an astoundingly sensitive formation that enables our perceptions, voluntary and involuntary movements, feelings, and thoughts. One of its essential support systems, analogous to plumbing, is called the ventricular system. As it circulates through a network of hollow caverns, or ventricles, CSF carries nourishment to the brain and takes waste away from it. The brain also floats buoyantly in a thin layer of CSF, which surrounds it inside the skull and spinal column and cushions it from impacts and the pressure of its own weight.
Cerebrospinal fluid is made deep inside the brain by the choroid plexus, a web-like formation of cells that extends into the ventricles. Fresh and nourishing CSF flows from the choroid plexus and circulates around the spinal cord and brain, bringing essential nutrients to the CNS’s cells. As it circulates, it also picks up the waste products given off by those cells. When it completes its course, the CSF carries waste out through small valves at the top of the brain called arachnoid granulations. From there, the fluid is re-absorbed by the bloodstream.
What causes pediatric hydrocephalus?
Several maladies can lead to hydrocephalus. A common one at or before birth is aqueductal stenosis, a condition in which the passage connecting two of the brain’s four major ventricles becomes too narrow for fluid to flow freely. Spina bifida and other spine disorders can also cause prenatal hydrocephalus. In addition to those congenital forms, hydrocephalus can also be acquired after birth. Head trauma, for example, is one common cause of acquired hydrocephalus. Another is infection. A prematurely born baby may also develop a bleed in the ventricles, called a germinal matrix hemorrhage, which may lead to hydrocephalus. Most cases of hydrocephalus, however, are called idiopathic, meaning that their cause is unknown.
Two main types of pediatric hydrocephalus
Doctors divide hydrocephalus into two main types: communicating and non-communicating. Think of the unimpeded flow of information that passes between people who are “communicating.” Similarly, in communicating hydrocephalus, there is an unimpeded flow of CSF between the different ventricles of the brain. The buildup of pressure in communicating hydrocephalus comes from an inability to absorb CSF. Now, think of the frustration caused when the flow of information between two people is impeded: they are “unable to communicate.” Similarly, in non-communicating hydrocephalus, the flow of CSF is impeded and backs up, causing a pathological increase in pressure.
Both kinds of hydrocephalus lead to a buildup of pressure inside the skull. In babies, whose cranial bones are not yet fully fused to one another, this pressure can force those bones apart, causing the head to grow abnormally large. In such cases, the fontanelles, or “soft spots,” on top of the head and between some of the main cranial bones, may bulge out noticeably. Other symptoms of hydrocephalus in newborns include swollen veins on the scalp, a protruding forehead and downward-pointing eyes, known as “sunset eyes,” that reveal unusually large whites above the irises.
How pediatric hydrocephalus is detected
A newborn’s head is typically measured at birth and again at each visit to the pediatrician. Abnormal head size, sometimes too subtle to perceive with the unaided eye, is the most frequent way hydrocephalus is discovered. However, a large head, also known as macrocephaly, does not necessarily mean a patient has hydrocephalus. In fact, macrocephaly is external hydrocephalus caused by benign subdurals of infancy. Unlike forms of hydrocephalus caused by increased CSF in the ventricles, the external form involves fluid outside the brain, usually does not require any treatment and typically resolves itself over time.
When a newborn is referred to a neurologist for indications of hydrocephalus, the first test is usually a cranial ultrasound. If the ultrasound shows enlarged ventricles, a radiologist will conduct a fast MRI to get a clearer picture of the causes. Depending on what the fast MRI reveals, it may then be necessary to conduct a full MRI, requiting sedation, to provide a level of detail that can guide decision-making about surgery.
Because the skull bones in older children have fused together, their heads do not enlarge, even with a significant increase of pressure in the brain. In these children, the first recognizable symptoms of hydrocephalus are often uncontrolled vomiting, lethargy, seizures or “sunset eyes.”
There are currently two main approaches to treating hydrocephalus. Whichever procedure is determined to be most promising for a particular patient, doctors at Lucile Packard Children’s Hospital are prepared to give them the best available treatment and long-term follow-up care.
Read about the main approaches to treating hydrocephalus, including an innovative new type of treatment called endoscopic third ventriculostomy, or ETV.

Connect with us:
Download our App: